 |
Research Article
Rehabilitation of a patient with spinal cord lesion due to surgical removal of the spinal tumor with chronic idiopathic demyelinating polyneuropathy (CIDP): A case report
1 Centre for the Rehabilitation of the Paralyzed (CRP), Savar, Dhaka, Bangladesh
2 Clinical Physiotherapist, Centre for the Rehabilitation of the Paralyzed, Dhaka, Bangladesh
Address correspondence to:
Md Zakir Hossain
Centre for the Rehabilitation of the Paralyzed (CRP), Savar, Dhaka,
Bangladesh
Message to Corresponding Author
Article ID: 100056D05MH2023
Access full text article on other devices

Access PDF of article on other devices


How to cite this article
Hossain MZ, Sohana A, Islam MW, Afridi S. Rehabilitation of a patient with spinal cord lesion due to surgical removal of the spinal tumor with chronic idiopathic demyelinating polyneuropathy (CIDP): A case report. Edorium J Disabil Rehabil 2023;9(2):15–22.ABSTRACT
Aims: The literature provides numerous medical therapies for chronic inflammatory demyelinating polyradiculoneuropathy (CIDP) and spinal cord lesion following spinal tumor surgery separately. Spinal cord injuries from CIDP-related spinal tumors have no evidence-based rehabilitation methods. This case report discusses CIDP, spinal cord lesion owing to a spine tumor, and tertiary care interdisciplinary rehabilitation. It shows how medical knowledge, clinical reasoning, and evidence guide outcome measures, care plans, and clinical decisions help to overcome CIDP.
Methods: In this report, we follow a 27-year-old male who began experiencing gradual paresthesia and mild weakening in his lower extremities for six weeks. After two months, the lumbar spine had the initial operation (laminectomy) because of the extreme pain. After the operation, he was pain-free, able to walk, and even started riding again. Pain in his lower midback, similar to cramping, and moderate swelling in his left ankle forced him into a wheelchair three years after his initial operation (intradural-extramedullary spinal space-occupying lesion at L2–L5 level). After the second operation (laminectomy), he had trouble in walking, lost sensation below the knees on both legs, and experienced mild incontinence. As the patient was confined to a wheelchair, he was standing with the help of two people. Significant main muscle group weakening was one of the first noticeable symptoms. Therapeutic exercise, balance training, functional training, and progressive endurance activities were the main components of the intervention. Berg balance score increased from 5 to 23, which is an eligible score for discharge.
Results: Clinical outcomes for the man with spinal cord lesion and chronic inflammatory demyelinating polyradiculoneuropathy (CIDP) were improved with interdisciplinary therapy. The patient underwent a first lumbar spine operation, which initially eased pain and allowed him to walk and ride again after feeling gradual paresthesia and minor weakened in his lower extremities.
Conclusion: For this patient with CIDP with spinal cord lesion due to spinal tumor, effective collaborative team communication and interdisciplinary management worked to optimize clinical decision making and recovery.
Keywords: Chronic inflammatory demyelinating polyneuropathy, Demyelinating conditions, Rehabilitation, Spinal tumor
Introduction
Intradural or extradural spinal tumors originate from the spinal cord or vertebrae. Intradural tumors are intramedullary, extramedullary, or both [1],[2],[3]. Most primary spinal cord cancers are schwannomas, generated from Schwann cells. Slow-growing, benign tumors can compress the spinal cord and nerve roots. Schwannomas are more common in the lumbar, thoracic, and cervical spine, and frequently detected after the age of 30 years. Chronic idiopathic demyelinating polyneuropathy (CIDP), an immune-mediated neuropathy, causes increasing weakening, sensory impairment, and missing or decreased tendon reflexes [4]. It occurs 0.67–10.3 times per 100,000 people [5]. Chronic idiopathic demyelinating polyneuropathy can be asymmetric, focal, or sensory/motor-dominated. European Federation of Neurological Societies/Peripheral Nerve Society 2010 CID diagnostic criteria are extensively utilized [6],[7]. Chronic idiopathic demyelinating polyneuropathy treatment tries to minimize inflammation, demyelination, and secondary axonal degeneration. Therapies continue until stabilization or maximum improvement [8]. Sensation, strength, and daily life gains indicate treatment efficacy. Infections, systemic disorders, and neurotoxic medications might worsen CIDP symptoms [9]. A 12-week aerobic or resistance exercises program for CIDP patients. The training program targeted specific muscle regions, whereas the aerobic program comprised regular cycling. Both exercise programs improved function and reduced symptoms [10]. Trauma, spinal degeneration, tumor compression, vascular disease, infection, and inflammation can cause spinal cord injury (SCI). Spinal cord injury treatment aims to improve symptoms, function, and long-term remission. Using the International Classification of Functioning, Disability, and Health (ICF) framework, physiotherapists can develop effective rehabilitation strategies for patients with neurological conditions by understanding the characteristics and management of spinal cord lesions with CIDP.
MATERIALS AND METHODS
The case has been selected conveniently in neurology unit of Centre for the Rehabilitation of the Paralyzed (CRP). The duration of observation was six months. The cases have been presented partially followed by case report (CARE) guideline and verbal consent has been taken from the patients and caregiver of the patients.
Case summary
Mr. Wahid, then 27 years old, began experiencing paresthesia and slight weakness in his lower limbs in 2013. He had suffered from lower back swelling ever since he was a kid, but he had managed to keep working through it. In 2013, however, he developed significant low back pain that rendered him bedridden; this ultimately led to lumbar spine surgery. The operation was fruitful, and he is now pain-free, mobile, and able to resume walking and cycling. The pain in Mr. Wahid’s lower midback and some moderate edema in his left ankle in 2016 rendered him wheelchair-bound once more. As a result, a second operation was required to remove an intradural-extramedullary spinal space-occupying lesion between lumbar levels L2 and L5. He developed slight bowel and bladder incontinence and was unable to walk following the second operation. Two people helped him to get up on his feet. Mr. Wahid’s symptoms worsened during the next six months, including upper- and lower-limb paresthesia and sleep jerking. Mr. Wahid had a hard time finding appropriate treatment for his symptoms despite the fact that he had no known medical disorders such diabetes, hypertension, thyroid issues, kidney disease, or heart disease. Following visits to the Neuroscience Hospital in Bangladesh and the Christian Medical College in India, among others, he was referred to physiotherapy specialists for further care and rehabilitation. In 2018, Mr. Wahid’s condition started to improve after 15 days of physiotherapy at Mymensingh Medical College Hospital. His rehabilitation showed promise and provided hope for more progress in the future, despite his ongoing reduced lower limb sensation, weakness in both legs, poor standing balance, urinary concerns, coordination challenges, and difficulty managing his stride.
Assessment
International Classification of Functioning, Disability, and Health (ICF) requires understanding disability state to improve a person’s quality of life [11]. Managing a person with any type of disability is multi-dimensional and comprehensive. The patient complained of significant weakness in both lower limbs and moderate weakness in the upper limb, modest upper limb pain, inability to stand, bladder problems, walking, and difficulties with activities of daily living (ADLs). His elbow pain, severe pelvic control, trunk control, wrist, and lower limb weakness with foot drop and moderate muscular wasting in tibialis anterior and surrounding the foot, gait irregularity, and upper limb fine motor activity were assessed. Visual analogue scale (VAS) pain was 6 out of 10 and decreased lower limb active range of motion (Hip Flexion 20°, abduction loss, 50° knee flexion present with knee extension full, ankle, foot movement in both lower limbs absent, upper limb range of motion is full). Lower limbs are withering. After two years, he went to physiotherapy. American Spinal Injury Association (ASIA) exam was his initial evaluation.
Instrumentation and tools
The American Spinal Injury Association assessed the case. This instrument is valid and reliable for measuring spinal cord injury neurological level and outcome [12]. CRP physiotherapy department neurology unit self-assessment is also included. Personal details included demographic information, history of present complaint, patient complaint, past medical history, medications, investigation, social history, home environment, general observations like consciousness, vision, hearing, edema, drooling, speech, subluxation, local observations like blood pressure, temperature, respiratory function, posture, upper and lower limb function uncompressing tonicity, sensation, and proprioception.
RESULTS
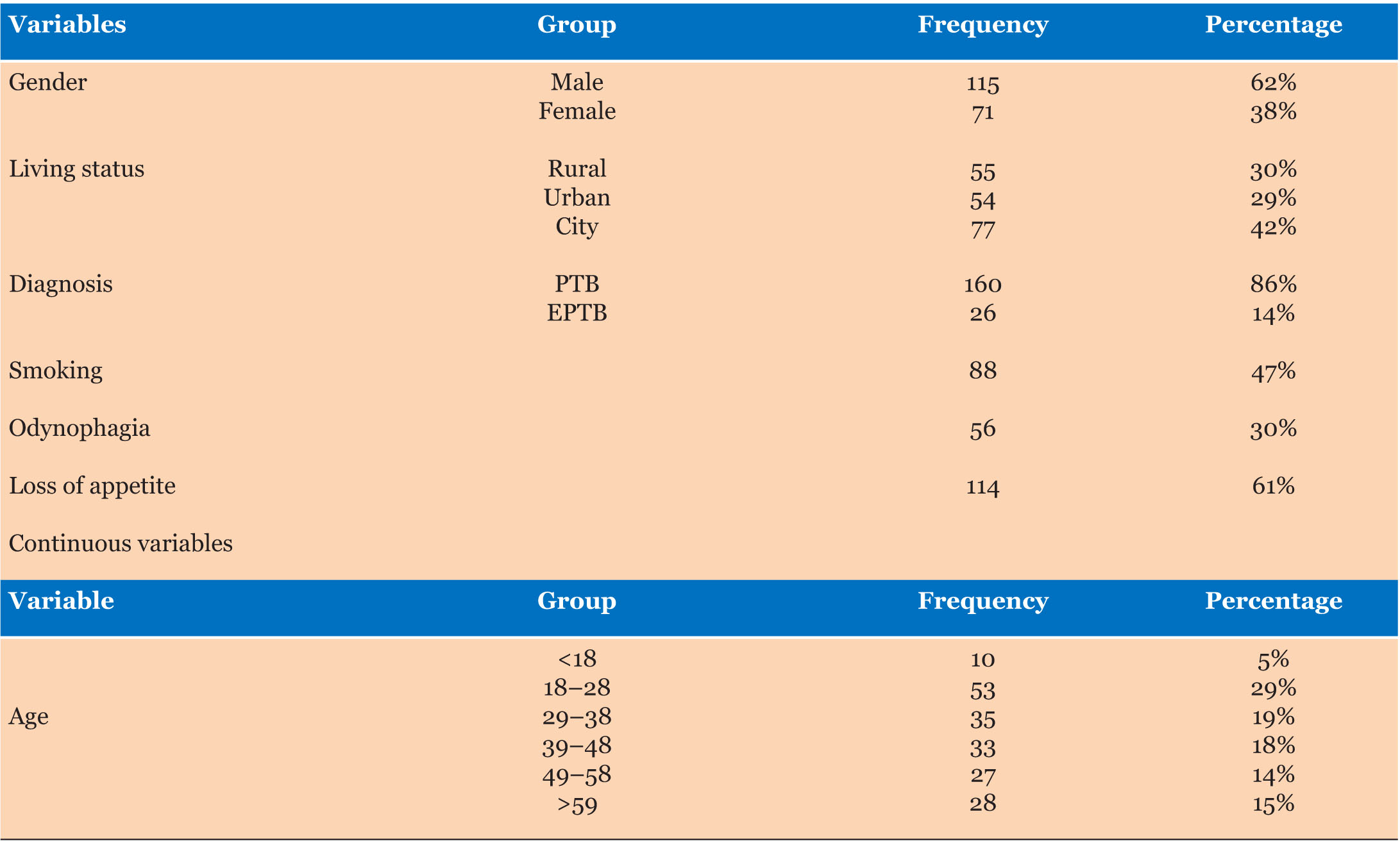
Clinical outcomes for the man with spinal cord lesion and chronic inflammatory demyelinating polyradiculoneuropathy (CIDP) were improved with interdisciplinary therapy. The patient underwent a first lumbar spine operation, which initially eased pain and allowed him to walk and ride again after feeling gradual paresthesia and minor weakened in his lower extremities. But by the age of 3 years, he was confined to a wheelchair due to lower midback pain and considerable swelling in his left ankle (Table 1). After undergoing a second procedure, the patient experienced slight incontinence, difficulty walking, and a loss of sensation below the knees (Table 2). Therapeutic exercise, balancing instruction, functional drills, and progressive endurance activities made up the rehabilitation intervention (Table 3).
The patient’s Berg balance score improved greatly from 5 to 23, making him a candidate for discharge (Table 4). When the interdisciplinary team worked together and communicated well, it helped guide clinical decision-making and speed the patient’s recovery (Table 5). This case report serves as a useful resource for future instances of a similar nature, highlighting the significance of evidence-based rehabilitation strategies in the management of spinal cord injury caused by CID-Prelated spine tumors (Figure 1).






Discussion
As each condition affects symptom management, treatment, rehabilitation, and prognosis, having a spinal cord lesion (SCL) from tumor removal and chronic inflammatory polyneuropathy (CIDP) can be devastating for patients and their families. In a study, spinal cord tumors are abnormal growths of tissue that can compress or invade the spinal cord or its surrounding structures, causing neurological deficits, pain, and disability and surgical removal of the tumor is often the primary treatment option, but it may also cause damage to the spinal cord or its blood supply, resulting in further impairment. The patient made minimal physical development in the first month of physiotherapy. His initial pain, low function, weak endurance, and mobility anxiety hampered physical therapy approaches. In a study, CIDP is a rare autoimmune disorder that causes progressive inflammation and demyelination of the peripheral nerves, leading to weakness, numbness, and sensory loss. Chronic idiopathic demyelinating polyneuropathy can coexist with spinal cord tumors, either as a paraneoplastic syndrome or as an incidental finding. Chronic idiopathic demyelinating polyneuropathy may also worsen the neurological outcome after spinal cord tumor surgery. The physical therapist’s supportive treatment, persistence, encouragement, and reinforcement of even tiny advances likely reduced functional deterioration and immobility, laying the groundwork for recovery. The physical therapist monitored the patient’s condition and implemented a flexible care plan using knowledge of CIDP and spinal cord damage and literature. Physical therapy is geared toward muscle strengthening, communication, and mobility. It may involve exercises, stretching, massage, electrical stimulation, hydrotherapy, and gait training. Medical therapies reversed the inflammatory process, allowing recuperation. Despite strength and endurance gains, the patient showed slow functional progress.
Conclusion
The development of standardized outcome measures and specific practice guidelines for CIDP with spinal cord lesion could lead to best-practice care for this condition.
REFERENCES
1.
Beall DP, Googe DJ, Mitchell BS. Intramedullary spinal cord tumors. The Surgical Clinics of North America 2007;87(5):1117–33.

2.
Chongyi F, Yonggang W, Xiaoguang L, Zhongjun L, Junming M, Qingsan Z. Analysis of the clinical symptoms and surgical treatment of 95 cases of intradural-extramedullary tumors. Journal of Clinical Neuroscience 2008;15(5):495–8.
3.
Arnautovic KI, Gokaslan ZL. Surgery for spinal tumors: Indications and techniques. Journal of Neuro-Oncology 2019;143(3):387–94.
4.
Elia-Pasquet S, Franques J, Devaux J, Fauchais AL, Blaison G. Chronic inflammatory demyelinating polyneuropathy. Revue Neurologique 2004;160(12 Pt 1):1223–30.
5.
Schellinger KA, Propp JM, Villano JL, McCarthy BJ. Descriptive epidemiology of primary spinal cord tumors. J Neurooncol 2008;87(2):173–9. [CrossRef]
[Pubmed]
6.
Sowash MG, Ballinger WE, Juel VC. Chronic inflammatory demyelinating polyneuropathy: An update on diagnosis and management. Clinical Neurology and Neurosurgery 2017;154:98–106.
7.
Milano E, Bianco M, Amoruso A, Di Sapio A, Sessa E, Toscano A. Chronic inflammatory demyelinating polyradiculoneuropathy: Diagnosis and treatment. Neurological Sciences 2010;31(5):573–81.
8.
Broers MC, Bunschoten C, Nieboer D, Lingsma HF, Jacobs BC. Guillain-Barré syndrome subtype diagnosis: A validation study. Journal of Neurology 2019;266(12):3064–70.
9.
Van den Bergh PY, Hadden RD, Bouche P, Cornblath DR. Peripheral nervous system involvement in immune-mediated diseases. Handbook of Clinical Neurology. Elsevier; 2010, Vol. 97, p. 663–80.
10.
Markvardsen LH, Overgaard K, Heje K, Sindrup SH, Christiansen I, Jensen TS. Aerobic training in patients with chronic inflammatory neuropathies: A randomized controlled trial. Brain and behavior 2017;7(3):e00649.
11.
Childs J, Blyth C, Pelletier C. Physiotherapy Management of Lower Limb Conditions: International Classification of Functioning, Disability, and Health (ICF). London: Elsevier Health Sciences; 2008.
12.
Marino RJ, Graves DE. Metric properties of the ASIA motor score: Subscales improve correlation with functional activities. Arch Phys Med Rehabil 2004;85(11):1804–10. [CrossRef]
[Pubmed]
13.
Ginis KM, Hicks AL, Latimer AE, et al. The development and testing of an exercise DVD for individuals with spinal cord injury. Spinal Cord 2018;56(9):836–43.
14.
Tse MA, Tang A, Baumgartner L, Weir PL, Inness EL, Jaglal SB. Physical activity programming in the rehabilitation of persons with spinal cord injury: Defining strategies for success. Spinal Cord 2018;56(3):225–33.
15.
Bye R, Pushman H, Summers J, et al. High-intensity resistance and functional training improve muscle strength, function, and disability in individuals with chronic incomplete spinal cord injury: A randomized controlled trial. J Neurotrauma 2017;34(1):23–9.
16.
Mehrholz J, Kugler J, Pohl M. Locomotor training for walking after spinal cord injury. Cochrane Database Syst Rev 2012;11:CD006676. [CrossRef]
[Pubmed]
SUPPORTING INFORMATION
Acknowledgments
The authors thank Md. KM Arman Hossain, Jashore Universiy of Science & Technology for his valuable suggestion and guidelines and also extend their heartful thanks to Md. Akhlasur Rahman, Junior consultant, Spinal Cord Injury Unit, CRP for his technical support.
Author ContributionsMd Zakir Hossain - Conception of the work, Design of the work, Acquisition of data, Analysis of data, Drafting the work, Revising the work critically for important intellectual content, Final approval of the version to be published, Agree to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Akter Sohana - Conception of the work, Design of the work, Acquisition of data, Drafting the work, Revising the work critically for important intellectual content, Final approval of the version to be published, Agree to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
MD Waliul Islam - Conception of the work, Design of the work, Acquisition of data, Analysis of data, Drafting the work, Final approval of the version to be published, Agree to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Shahid Afridi - Conception of the work, Design of the work, Acquisition of data, Analysis of data, Drafting the work, Revising the work critically for important intellectual content, Final approval of the version to be published, Agree to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Guaranter of SubmissionThe corresponding author is the guarantor of submission.
Source of SupportNone
Consent StatementWritten informed consent was obtained from the patient for publication of this article.
Data AvailabilityAll relevant data are within the paper and its Supporting Information files.
Conflict of InterestAuthors declare no conflict of interest.
Copyright© 2023 Md Zakir Hossain et al. This article is distributed under the terms of Creative Commons Attribution License which permits unrestricted use, distribution and reproduction in any medium provided the original author(s) and original publisher are properly credited. Please see the copyright policy on the journal website for more information.



{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}