 |
Research Article
Fall-related self-efficacy in adults poststroke: A cross-sectional study
1 Physiotherapist, Habiliteringen Region Kalmar, County Hospital Kalmar, Kalmar, Sweden
2 Associate Professor, Department of Neuroscience, Rehabilitation Medicine, Uppsala University, Uppsala, Sweden
Address correspondence to:
Jessica Söderborg
Vallmovägen 2, 385 51 Söderåkra,
Sweden
Message to Corresponding Author
Article ID: 100047D05JS2019
Access full text article on other devices

Access PDF of article on other devices


How to cite this article
Söderborg J, Hellström K. Fall-related self-efficacy in adults poststroke: A cross-sectional study. Edorium J Disabil Rehabil 2019;5:100047D05JS2019.ABSTRACT
Aims: The overall aim was to describe and examine if there is a difference between men and women in fall-related self-efficacy (SE). Another aim was to examine the strength of associations between fall-related SE and physical function and health-related quality of life (QoL) in community-living individuals poststroke.
Methods: A cros-ssectional study was conducted within two weeks of admission to rehabilitation or first week follow-up after discharge from hospital. Used tests were fall-related self-efficacy (FES-S), Functional Ambulation Classification (FAC), 10 meter walking test (10 mWT), the functional independence measure (FIM), and health-related QoL (EQ5D). The analysis was based on 37 individuals with a mean age off 68.5 years.
Results: The results showed that physical factors but not QoL had association with perceived confidence in task performing without falling. No gender difference was shown.
Conclusion: In this study physical function was associated with fall-related SE.
Keywords: Fall-related self-efficacy, Gender, Physical function, Poststroke, Quality of life
Introduction
In industrialized populations, stroke is a common cause of death and long-term disability [1]. In Sweden approximately 21,000 individuals suffer from a stroke each year. At the time of the stroke the mean age for men is 73 years and for women 78 years [2]. In the past decades there have been a strong decline in stroke mortality and long-term survival after stroke continues to improve. Due to the growing elderly population this results in an increased number of individuals in Sweden who previously have had a stroke. In Sweden approximately every sixth individual who suffered a stroke will have a long-term disability [2]. The symptoms after stroke are varied and depend on which part of the brain is injured and how severely it is affected [3]. Often the symptoms are on one side of the body and the most common symptoms are weakness or numbness, loss and/or disturbance of motor function, cerebral visual impairment, difficulty in communication, and reduced cognitive function [3]. Pound et al. [4] suggest that the most disabling consequence of stroke is the loss of independent ambulation as it affects almost every aspect of daily living [4]. In community-dwelling stroke survivors, walking is the most frequent activity leading to falls with a rate of 39–90% [5]. In community ambulation gait speed is important for individuals poststroke [6]. Self-selected gait speed <1m/s can identify older people at risk for health-related outcomes [7]. as it is one risk factor for falling [5]. Studies have shown that individuals poststroke have a risk of falling that is significantly higher than that of age- or gender-matched controls. The proportions of fallers range from 23% to 34% (3–4 month follow-up), 40% to 73% (6 month follow-up), and 43% to 70% (1 year follow-up) in community-dwelling stroke survivors [5]. Stroke group characteristics can partly explain the difference in fall incidence rates [5]. Falls can lead to a variety of physical and psychosocial consequences. One severe physical consequence is hip fracture with an odds ratio of 2.1 (aged >80), 3 (70–80), and 3.8 (>70) for individuals poststroke [5]. Furthermore, surgically treated hip fractures have a doubled mortality rate in individuals poststroke. The psychosocial consequences of falls are equally important [5]. Many individuals develop fear of falling (FoF) [5],[8], defined as “persisting concern regarding falling” [9]. Studies have shown that FoF is associated with restriction in mobility/activity, reduced social interactions, and poor QoL [5]. Reduction in QoL is associated with further declines in physical, psychological, and mental functions [5].
Stroke rehabilitation is essential to minimize long-term loss of function and the rehabilitation is multifaceted [10]. Physical therapists working in stroke rehabilitation play an active role in motor skills learning or relearning voluntary control over the affected muscles [10]. Bandura’s social cognitive learning theory (SCT) [11] is a well-developed theory that elucidates the underlying mechanisms involved in maximizing learning. Social cognitive learning theory points out the interaction between the individual, the environment, and the behavior [11]. Self-efficacy is a central concept in SCT and is defined as the degree of confidence a person has in his/her ability to perform specific behaviors successfully. Individuals with high SE approach the particular activity with confidence and individuals with low SE tend to avoid the activity [12]. Those SE beliefs are thought to be domain specific; they pertain to a specific behavior in a particular context and do not necessarily generalize to other behaviors or other contexts [11],[13]. Self-efficacy is a psychological construct which predicts both QoL [14],[15], mobility [15], and activities of daily living poststroke [15],[16], and several studies have found that SE is a strong predictor of real-world walking activity [16],[17],[18]. The use of SE can help the individual during the rehabilitation to gain more control of important aspects of their disease [15]. Therefore, it is of importance that physiotherapy takes into account the individuals SE toward the task during rehabilitation. Four main sources can develop SE: (1) mastery experience, successfully performing a task, (2) vicarious experience of a task (the individual is observing others performing the task), (3) verbal persuasion/encouragement, and (4) psychological state (anxiety and depression) [15]. There can however be a challenge measuring SE in individuals with cognitive and/or language impairment due to the difficulty in grasping the concept of rating confidence levels [18].
Assessment of stroke impacts on daily living should include physical, psychological, and social consequences [19] because individuals poststroke can be confronted with limitations in all three aspects [15]. Therefore, it is of importance to develop better understanding of the relationship between SE and physical function and QoL as it can have an impact on how training poststroke is planned, particularly within the field of physiotherapy.
Aim
This study had four purposes: (1) To describe fall-related SE, (2) and to examine if there was a difference between men and women with stroke in fall-related SE.
To investigate the strength of association between (3) fall-related SE and physical function and (4) fall-related SE and health-related QoL.
MATERIALS AND METHODS
Participants
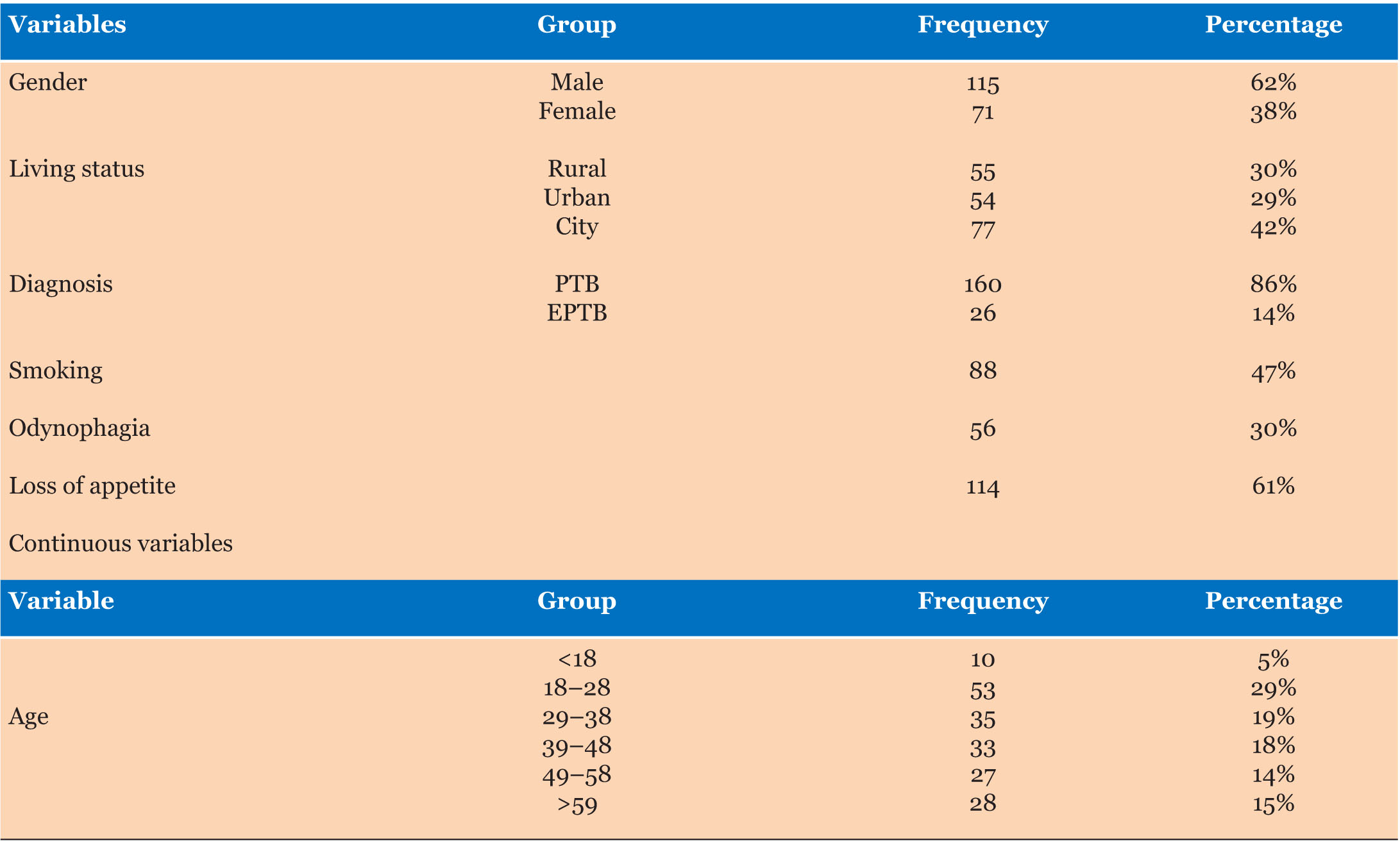
During a period of approximately two years 37 participants, 18 men and 19 women, were consecutively included in the study. Table 1 provides data on demographics and stroke characteristics.
In order to achieve a breadth of the study, the recruitment was done from all six daycare rehabilitation centers within the area of Gävle Hospital and from Gävle Hospital “home follow up team.” To be included in the study, the individual had to be an adult and have limitations in physical functioning requiring rehabilitation due to stroke. A few did not want to participate and a number of individuals were not asked due to exclusion criteria (could not understand FES-S or EQ5D and/or already participated in rehab during last six months). Unfortunately there is no record of how many individuals who were excluded or did not want to participate.
Assessment instruments
Demographics data and stroke characteristics included: sex, age, respectively, stroke type, affected side, weeks since stroke, fall history (self-reported fall to the ground), previous rehab, and where recorded by questionnaire.
The Falls Efficacy Scale-Swedish version (FES-S) is a visual analog scale measuring fall-related SE in 13 items common in everyday life [20]. It is divided into two subscales: Personal activities of daily living (PADL) and instrumental activities of daily living (IADL), and an in-between item (walking up and down stairs). The score range from 0 (not confident) to 10 (completely confident) gives a total score of 130. Falls Efficacy Scale-Swedish version has an acceptable test–retest reliability (K = 0.97) and validity in individuals with stroke [20],[21].
Functional Ambulation Classification (FAC) scale distinguishes six levels of walking ability based on the amount of physical support required, score range from 0 (nonfunctional ambulator) to 5 (ambulator independent) [22]. The reliability of FAC is described in studies with different results. The most recent study from Mehrholz et al. [23] shows that FAC has high test–retest reliability (K = 0.95) and interrater reliability (K = 0.905) in individuals with stroke.
Ten meter walking test (10 mWT) measures selfselected gait speed m/s over 10 m with a stop watch. The test is done in a straight line and without a cognitive task. Slow walking speed <1.0 m/s. Individuals who experienced a stroke the test has acceptable psychometric properties [24].
The functional independence measure (FIM) scale is an 18-item instrument measuring activities of daily living and it is divided into two subscales: motor function and cognitive function. The score range from 1 (complete dependence) to 7 (independence) gives a total score of 126. The FIM scale has well-established reliability and validity [25],[26].
EuroQol five dimension questionnaire (EQ5D) and visual analogue scale (EQ-VAS). Measuring healthrelated QoL (EQ5D) by assessing five items: mobility, self-care, usual activities, pain/discomfort, and anxiety/depression. Each with a three level rating scale: Level 1 indicates no problem, level 2 indicates some problems, and level 3 indicates extreme problems. EuroQol-visual analogue scale starts from 0 (lowest QoL) to 100 (highest QoL). The test is valid and reliable in individuals who have experienced a stroke [27],[28].
Procedure
The study was cross-sectional and completed in accordance with the Swedish law of Ethical Review [29]. No ethical application was made due to the fact that there was no intervention in the study. The individuals were asked to participate in the study by their treating physiotherapist or occupational therapist. Oral and written information about the study was given and the individuals were informed that they could withdraw their approval at any time. Written informed consent was provided by all participants and all material was coded.
The therapists had written and oral information about the assessment instruments. The tests were not done in a certain order. All participants were assessed within two weeks of admission to daycare rehabilitation center or first week follow-up after discharge from Gävle hospital (“home follow up team”). They were mainly assessed by their treating physiotherapists, and some participants were also assessed by their treating occupational therapist. If the patient had aphasia a speech therapist helped with the questionnaires (FES-S and EQ5D).
Statistical analysis
To describe fall-related SE a power computation of the null hypothesis was done with Fisher’s Z approximation before the start of the study. The criterion for significance (alpha) was set at 0.050, with a power of 90%. Thirty-four participants were needed. To investigate the association between fall-related SE and physical function, and fall-related SE and QoL, a precision computation was done. Based on the same parameters and assumptions the study will report the value with a precision (95% confidence level) of approximately ±0.3 points.
Demographics, stroke characteristics, and study parameters were calculated and described with descriptive statistics. To evaluate the relations between FES-S and physical function and perceived health status Spearman’s correlation (rho) was used and Cohen’s conventions for small (0.1), medium (0.3), or large (0.5) effect size. The Mann–Whitney U test was used to identify group difference between men and women. Statistical significance at p < 0.05 was assumed throughout. All analyses were performed using statistical Package for Social Services (SPSS) computer program.

RESULTS
Fall-related self-efficacy
Overall rating of FES-S (total score) was high with a median score of 112.5 for men and 120 for women. The FES-S (total score and subscales) did not show any difference between men and women (p > 0.05) in fallrelated SE. The median score, interquartile range, and range for the FES-S (total score and subscales) and the p value to identify possible group difference are presented in Table 2.
Physical function
The FIM scale, FAC scale, and 10 mWT had statically strong significant association with the FES-S (p < 0.05) (Table 3). Median scores, interquartile range and range for the FIM scale, FAC scale, and 10 mWT are presented in Table 4.
Quality of life
The EQ5D VAS was not associated with the FES-S (p > 0.05) (Table 3). Median score, interquartile range, and range of the EQ5D VAS are presented in Table 5. The scoring in the dimensions is also presented in Table 5.




Discussion
The overall rating of FES-S was high with a median score of 120 for women and 112.5 for men. The individuals reported on the EQ5D dimensions mobility and usual activity level 2 (indicating some problems) whereas in self-care level 1 (indicating no problems) showed the highest response rate. That in combination with the hightest scores in FAC and FIM (total and subscales) indicates high functioning individuals in this study.
In comparison with other studies in the stroke population [8],[16],[30], the present study showed that physical function was associated with fall-related SE. As suggested by the SE theory, the relationship between efficacy and function may be reciprocal. Efficacy may influence function, while at the same time function may influence efficacy [12]. This is confirmed by existing literature with studies showing that SE is a significant predictor of physical function [16],[18] including balance [30],[31], gait capability [30], level of physical activity [32], and fall history [30],[31]. The study by Andersson et al. [8] showed a significant association between low fallrelated SE and impaired physical function in individuals poststroke who had fallen and in those who had not.
Furthermore, there was a low rate of falling (Table 1); 33.3% for men and 36.8% for women, compared with other studies [5]. The high level of functional independence may have contributed to this. In a high functioning population with stroke a fall rate of 40% is still occurring [31]. The high risk of falling is a considerable health concern [5]. One risk for falling is slow walking speed [5],[33]. Persson et al. [33] showed that self-selected gait speed at ≤1.2 m/s on the 10 mWT tested one week after stroke increased the risk for falling during the first year and those individuals who were unable to perform the test had the highest risk. In healthy adults the mean self-selected gait speed is 1.33 m/s for men and 1.27 m/s for women [34]. The present study showed a mean self-selected gait speed of 0.9 m/s in both men and women. Previous studies have reported similar results with slower self-selected gait speed in a population with stroke [5],[32],[35] with velocities ranging from 0.66 to 1.2 m/s [6]. In community ambulation a gait speed at more than 1.2 m/s is needed to cross a street safely [36].
Different approaches to assess FoF have been developed over the years [37] and the Fall Efficacy Scale was one of them [13]. While some authors may suggest that fall-related SE and FoF are the same, but we do not agree. While related, fall-related SE and FoF are distinct constructs [37]. Fall-related SE is defined as “perceived confidence in task performing without falling” [21] and FoF is defined “persisting concern regarding falling” [9]. Nevertheless, several studies have used the SE theory to evaluate FoF [18],[19],[38]. Kim et al. [38] found an association, similar to ours, between FAC and FoF measured with the Korean version of falls efficacyscale in subacute stroke patients. Fall-related SE and FoF have however been found to be correlated given the relationship between fear and beliefs [37]. Low fallrelated SE and FoF can restrict performance of daily living [13] but on the other hand some level of FoF can promote effective coping skills for prevention of falls [19].
In the literature there has been some discussion of the influence of sex on SE. Some author’s hypothesis is that men rate higher SE due to a higher educational level, occupational status, monthly income, or social influence. Other authors suggested that men rate higher SE in stroke rehabilitation to offer an image of strength and control [18]. This study did not show a significant difference between men and women in fall-related SE. Some studies showed the same results [21], yet others suggested that men rate a higher SE than women [18]. In our results, although not a significant difference, the women rated a higher SE than the men. The women did however also a slightly higher median score in FIM and FAC test have.
The participants in this study had a high median score of the FIM subscale that includes aspects of cognitive function. There has been some discussion of the influence of cognitive and/or perceptual impairments on SE. Bandura [12] suggests that individuals with cognitive impairments have limited ability to process information drawn from positive experiences that should enhance SE [12]. The study by Hellström and Lindmark [21] did not show any significant difference in FES-S scores in any of the 13 items between individuals poststroke with or without cognitive and perceptual impairments [21]. Previous studies have shown that when motor function, cognition, and psychosocial capacity are reasonable intact, poststroke performance-based mobility may be significantly limited due too poor SE [17],[32].
In contrast to some previous studies, ours did not show any association between fall-related SE [38] and QoL. Furthermore, earlier studies have suggested that there is a difference between men and women, where women more frequently rate lower on QoL and depression [39]. While this study, like the one from Andersson et al. [8], did not show any significant difference, it could however indicate a difference between men and women regarding QoL and depression. EuroQol-visual analogue scale mean was at 65 for men and 50 for women, and the highest percentage in dimension anxiety/depression was level 1 for men at 61.1% and level 2 for women at 47.4%.
The results in this study support the concept of using SE within the field of physical therapy in stroke rehabilitation to help the individual to gain better function in activities of daily living post stroke.
Limitations
There were several methodological limitations to the study. It was a cross-sectional study, so predictive relationships cannot be drawn. Among the participants in this study, there are both individuals who have fallen and not fallen, those who have received rehabilitation before due to a previous stroke and those who have not received it. It can affect the test result as the group is not homogeneous. That does however form a group of individuals with which many rehabilitation staff will be familiar with. Furthermore, the women of the study had a lower mean age at 65 years compared with 78 years overall in Sweden. Also the study sample was likely representative of highly functioning individuals. It should be emphasized that the study sample was quite small.
Conclusion
In this study different measures of physical function stood out as the most important variable associated with the fall-related SE. Consequently, the hypothesis that QoL is associated with fall-related SE that is not supported by the present study. Furthermore, no difference between men and women in fall-related SE is shown.
REFERENCES
1.
Feigin VL, Lawes CM, Bennett DA, Andersson CS. Stroke epidemiology: A review of population-based studies of incidence, prevalence, and case-fatality in the late 20th century. Lancet Neural 2003;2(1):43–53. [CrossRef]
[Pubmed]

2.
Riksstroke the Swedish stroke register. [Available at: http://www.riksstroke.org/eng/]
3.
Health topics: Stroke, Cerebrovascular accident. Geneva: World Health Organization; 2017.
4.
Pound P, Gompertz P, Ebrahim S. A patient-centered study of the consequences of stroke. Clin Rehabil 1998;12(4):338–47. [CrossRef]
[Pubmed]
5.
Weerdesteyn V, de Niet M, van Duijnhoven HJ, Geurts AC. Falls in individuals with stroke. J Rehabil Res Dev 2008;45(8):1195–213. [CrossRef]
[Pubmed]
6.
van de Port IG, Kwakkel G, Lindeman E. Community ambulation in patients with chronic stroke: How is it related to gait speed? J Rehabil Med 2008;40(1):23–7. [CrossRef]
[Pubmed]
7.
Cesari M, Kritchevsky SB, Pinninx BW, et al. Prognostic value of usual gait speed in well-functioning older people—results from the health, aging and body composition study. J Am Geriatr Soc 2005;53(10):1675–80. [CrossRef]
[Pubmed]
8.
Andersson AG, Kamwendo K, Appelros P. Fear of falling in stroke patients: Relationship with previous falls and functional characteristics. Int J Rehabil Res 2008;31(3):261–4. [CrossRef]
[Pubmed]
9.
Tinetti ME, Powell L. Fear of falling and low self-efficacy: A case of dependence in elderly persons. J Gerontol 1993;48:35–8. [CrossRef]
[Pubmed]
10.
Langhorne P, Coupar F, Pollock A. Motor recovery after stroke: A systematic review. Lancet Neurol 2009;8(8):741–54. [CrossRef]
[Pubmed]
11.
Bandura A. Self-efficacy: Toward a unifying theory of behavioral change. Psychol Rev 1977;84(2):191–215. [CrossRef]
[Pubmed]
12.
Bandura A. Self-efficacy mechanism in human agency. Am Psychol 1982;37:122–47.
13.
Tinetti ME, Richman D, Powell L. Falls efficacy as a measure of fear of falling. J Gerontol 1990;45(6):P239–43. [CrossRef]
[Pubmed]
14.
LeBrasseur NK, Sayers SP, Ouellette MM, Fielding RA. Muscle impairments and behavioral factors mediate functional limitations and disability following stroke. Phys Ther 2006;86(10):1342–50. [CrossRef]
[Pubmed]
15.
Korpershoek C, van der Bijl J, Hafsteinsdóttir TB. Self-efficacy and its influence on recovery of patients with stroke: A systematic review. J Adv Nurs 2011;67(9):1876–94. [CrossRef]
[Pubmed]
16.
Hellström K, Lindmark B, Wahlberg B, Fugl-Meyer AR. Self-efficacy in relation to impairments and activities of daily living disability in elderly patients with stroke: A prospective investigation. J Rehabil Med 2003;35(5):202–7. [CrossRef]
[Pubmed]
17.
Dansk KA, Pohlig RT, Roos M, Wright TR, Reisman DS. Relationship between walking capacity, biopsychosocial factors, self-efficacy, and walking activity in persons poststroke. J Neural Phys Ther 2016;40(4):232–8. [CrossRef]
[Pubmed]
18.
Salbach NM, Mayo NE, Robichaud-Ekstrand S, Hanley JA, Richards CL, Wood-Dauphinee S. Balance self-efficacy and its relevance to physical function and perceived health status after stroke. Arch Phys Med Rehabil 2006;87(3):364–70. [CrossRef]
[Pubmed]
19.
Hellström K, Lindmark B, Fugl-Meyer A. The falls-efficacy scale, Swedish version: Does it reflect clinically meaningful changes after stroke? Disabil Rehabil 2002;24(9):471–81. [CrossRef]
[Pubmed]
20.
Hellström K, Nilsson L, Fugl-Meyer A. Relationship of confidence in task performance with balance and motor function after stroke. Physiotherapy Theory and Practice 2001;17(2):55–65. [CrossRef]
21.
Hellström K, Lindmark B. Fear of falling in patients with stroke: A reliability study. Clin Rehabil 1999;13(6):509–17. [CrossRef]
[Pubmed]
22.
Holden MK, Gill KM, Magliozzi MR, Nathan J, Piehl-Baker L. Clinical gait assessment in the neurologically impaired. Reliability and Meaningfulness. Phys Ther 1984;64(1):35–40. [CrossRef]
[Pubmed]
23.
Mehrholz J, Wagner K, Rutte K, Meissner D, Pohl M. Predictive validity and responsiveness of the functional ambulation category in hemiparetic patients after stroke. Arch Phys Med Rehabil 2007;88(10):1314–9. [CrossRef]
[Pubmed]
24.
Tyson S, Connell L. The psychometric properties and clinical utility of measures of walking and mobility in neurological conditions: A systematic review. Clin Rehabil 2009;23(11):1018–33. [CrossRef]
[Pubmed]
25.
Cifu DX, Stewart DG. Factors affecting functional outcome after stroke: A critical review of rehabilitation interventions. Arch Phys Med Rehabil 1999;80(5 Suppl 1):S35–9. [CrossRef]
[Pubmed]
26.
Functional Independence Measure. Vägledning. Version 5.0. Svensköversättning. u.o.: Uniform Data System for Medical Rehabilitation, a division of U B Foundation Activities, INC, 1996.
27.
Dorman PJ, Waddell F, Slattery J, Dennis M, Sandercock P. Is the EuroQol a valid measure of health-related quality of life after stroke? Stroke 1997;28(10):1876–82. [CrossRef]
[Pubmed]
28.
Dorman P, Slattery J, Farrell B, Dennis M, Sandercock P. Qualitative comparison of the reliability of health status assessments with the EuroQol and SF-36 questionnaires after stroke. United Kingdom Collaborators in the International Stroke Trial. Stroke 1998;29(1):63–8. [CrossRef]
[Pubmed]
30.
Rosén E, Sunnerhagen KS, Kreuter M. Fear of falling, balance, and gait velocity in patients with stroke. Physiother Theory Pract 2005;21(2):113–20. [CrossRef]
[Pubmed]
31.
Belgen B, Beninato M, Sullivan PE, Narielwalla K. The association of balance capacity and falls self-efficacy with history of falling in community-dwelling people with chronic stroke. Arch Phys Med Rehabil 2006;87(4):554–61. [CrossRef]
[Pubmed]
32.
Vahlberg B, Cederholm T, Lindmark B, Zetterberg L, Hellström K. Factors related to performance-based mobility and self-reported physical activity in individuals 1–3 years after stroke: A cross-sectional cohort study. J Stroke Cerebrovasc Dis 2013;22(8):e426–34. [CrossRef]
[Pubmed]
33.
Persson CU, Hansson PO, Sunnerhagen KS. Clinical tests performed in acute stroke identify the risk of falling during the first year: Postural stroke study in Gothenburg (POSTGOT). J Rehabil Med 2011;43(4):348–53. [CrossRef]
[Pubmed]
34.
Bohannon RW. Comfortable and maximum walking speed of adults aged 20–79 years: Reference values and determinants. Age Ageing 1997;26(1):15–9. [CrossRef]
[Pubmed]
35.
Vahlberg B, Cederholm T, Lindmark B, Zetterberg L, Hellström K. Short-term and long-term effects of a progressive resistance and balance exercise program in individuals with chronic stroke: A randomized controlled trial. Disabil Rehabil 2017;39(16):1615–22. [CrossRef]
[Pubmed]
36.
Langlois JA, Keyl PM, Guralnik JM, Foley DJ, Marottoli RA, Wallace RB. Characteristics of older pedestrians who have difficulty crossing the street. Am J Public Health 1997;87(3):393–7. [CrossRef]
[Pubmed]
37.
Hadjistavropoulos T, Delbaere K, Fitzgerald TD. Reconceptualizing the role of fear of falling and balance confidence in fall risk. J Aging Health 2011;23(1):3–23. [CrossRef]
[Pubmed]
38.
Kim EJ, Kim DY, Kim WH, et al. Fear of falling in subacute hemiplegic stroke patients: Associating factors and correlations with quality of life. Ann Rehabil Med 2012;36(6):797–803. [CrossRef]
[Pubmed]
39.
Appelros P, Stegmayr B, Terént A. A review on sex differences in stroke treatment and outcome. Acta Neurol Scand 2010;121(6):359–69. [CrossRef]
[Pubmed]
SUPPORTING INFORMATION
Acknowledgments
The authors would like to thank all the participants involved. We would also like to express our appreciation to physiotherapist Maria Svedjebrant and her colleagues at County Hospital, Gävle, Sweden. The study would not have been possible without their assistance. Thanks to Kristofer Årestedt, professor and research leader for the iCARE group for help with the analysis. This study was supported in part by grants from “Fysioterapeuternas Minnesfond.”
Author ContributionsJessica Söderborg - Conception of the work, Design of the work, Acquisition of data, Analysis of data, Drafting the work, Revising the work critically for important intellectual content, Final approval of the version to be published, Agree to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Karin Hellström - Conception of the work, Design of the work, Drafting the work, Revising the work critically for important intellectual content, Final approval of the version to be published, Agree to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Guaranter of SubmissionThe corresponding author is the guarantor of submission.
Source of SupportNone
Consent StatementWritten informed consent was obtained from the patient for publication of this article.
Data AvailabilityAll relevant data are within the paper and its Supporting Information files.
Conflict of InterestAuthors declare no conflict of interest.
Copyright© 2019 Jessica Söderborg et al. This article is distributed under the terms of Creative Commons Attribution License which permits unrestricted use, distribution and reproduction in any medium provided the original author(s) and original publisher are properly credited. Please see the copyright policy on the journal website for more information.


{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}